
By Chris Faubel, MD —
Background
- Carpal tunnel syndrome is a peripheral entrapment mononeuropathy of the median nerve as it courses through the carpal tunnel.
- Local compressive entrapment causes demyelination leading to nerve block (neuropraxia). If the compression persists, local nerve blood flow decreases (vasa nervorum) leading to a cascade of events eventually causing axon damage (axonotmesis).
- The pain is thought to result from inflammatory mediators (TNFα) causing abnormal Na+ influx into these damaged nociceptive fibers.
Epidemiology
- Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy.
- A Swedish general population survey in 1999 [1] showed 14.4% of responders reported numbness and/or tingling in the median nerve distribution, although only 1 in 5 (20%) symptomatic subjects were found to have clinically AND electrodiagnostically confirmed CTS.
- The overall prevalence was said to be 2.7% — of CTS confirmed by clinical exam and nerve conduction studies
- A US survey conducted in 1988 [2] showed an estimated 1.88% of the general population had self-reported carpal tunnel syndrome, with females and whites having the highest prevalence
- Certain occupations have been shown to have a much higher prevalence of CTS than the general population
- Female supermarket checkers: prevalence = 62.5% (self-reported symptoms only) [3]
- Mail service, health care, construction, and assembly and fabrication. [4]
- Risk factors (most strongly associated with CTS) [4]
- Repetitive bending/twisting of the hands/wrists at work (OR = 5.2) [OR = odds ratio]
- Race (OR = 4.2; WHITES higher than nonwhites)
- Gender (OR = 2.2; FEMALES higher than males)
- Use of vibrating hand tools (OR = 1.8)
- Age (OR = 1.03; risk increasing per year)
- Wrist ratio (A-P:med-lat) – If the anterior to posterior distance is ≥70% of the medial to lateral distance, there is a significant association with idiopathic CTS. [30]
- High body mass index (BMI) – obesity [38]
- Keyboard Use and CTS
- Some studies have shown no association between computer use and carpal tunnel syndrome. [31] [32]
- Another study found that workers who identified themselves as “intensive keyboard users” had less CTS than the control group. [34]
- A big problem with this study was that the control group had a significantly greater number of manual laborers with jobs that required repetitive twisting/bending of the wrists (the number one risk factor above).
- The question of whether intense keyboard use (i.e., >4 or >6 hours per day) is associated with an increased or decreased risk of CTS is still unanswered. [33]
- Bilateral CTS [29]
- 87% of patients with CTS, have electrodiagnostic (EDX) abnormalities bilaterally.
- 50% of asymptomatic hands have EDX findings of CTS.
- Most cases of unilateral CTS developed symptoms in the contralateral hand over time.
- Duration of symptoms, not severity of symptoms, positively correlated with developing bilateral CTS.
- Pregnancy
- Carpal tunnel syndrome is common during pregnancy.
- Wearing a night-time wrist splint helps reduce the pain for a week, but then it stays the same until delivery. [35]
- Pain cuts in half during the first week after delivery, then half again the next week. [35]
- Pain reduction strongly correlated with weight loss after delivery.
- Symptoms frequently persist after delivery
- More than 50% of the patients after 1 year and in about 30% after 3 years [36]
- Corticosteroid injections provide significant relief [37]
- 4 mg of dexamethasone acetate was used in the third trimester.
- A month after delivery, both the injected and non-injected hands had symptom improvement.
Clinical Features
- CTS can be thought of as occurring in three stages
- First stage
- Nocturnal sensations of hand swelling, numbness/tingling (in the median nerve distribution), and pain that frequently is felt all the way up to the ipsilateral shoulder.
- Patients may report that shaking their hands helps.
- Hand stiffness in the morning
- Second stage
- Same symptoms, but now during the day; mostly when the patient’s wrist remains in the same position too long, or with repetitive wrist movements.
- Dropping objects — patients may start reporting that they drop objects because of hand weakness.
- Third stage
- Noticeable thenar muscle atrophy.
- Note: sensory complaint are now much less, or even completely absent.
- First stage
- Paresthesia distribution in the hand [39]
- 70.4% of patients with CTS present with whole hand distribution of paresthesias
- 29.6% present with paresthesias strictly in the median nerve distribution
- Patients suffering from severe CTS were more likely to have median nerve distribution symptoms.
- Severity of symptoms vs NCS findings
- No statistically significant relationship between the severity of symptoms a patient has, and the severity of electrodiagnostic findings. [40]
Diagnosis
- Important history (to get from the patient)
- Symptom onset (night vs day)
- Provocative factors (certain positions; repeated movements)
- Occupation (wrists movements; vibratory tools)
- Pain localization (median distribution; ascending to shoulder; descending from shoulder)
- Alleviating maneuvers (shaking out hands; position changes)
- Predisposing factors (diabetes, obesity, acromegaly, pregnancy, polyarthritis)
- Sports/activites (baseball; body-building)
- Physical examination
- Katz hand diagram (click here for image)
- A patient is given a sheet of paper with outlined palmar and dorsal hands, and is asked to fill in the areas where they experience symptoms (pain; numbness; tingling).
- The physician then looks at the filled out diagram and classifies it as “classic“, “probable“, and “unlikely“.
- It was originally thought to correlate well with whether the patient will have electrodiagnostically-confirmed CTS. [5]
- A recent study in 2010 [6] had two hand surgeons evaluate 75 diagrams (filled out by patients with CTS and other pathologies) at two occasions 4-weeks apart.
- Inter-rater agreement was poor and intra-rater agreement was fair, making this test unreliable and inconsistent.
- Tinel’s test (at the wrist)
- Tapping over the median nerve directly over the carpal tunnel, or just proximal
- Sensitivity = 67%, Specificity = 68% [8]
- Very little diagnostic value in CTS
- More likely to be positive in the later stages of nerve compression [7]
- Phalen’s test
- Static wrist flexion for 60 seconds (or until symptoms)
- Sensitivity = 85%, Specificity = 89% [8]
- Positive mostly in moderate to severe CTS [41]
- Hypalgesia in the median nerve distribution
- Sensitivity = 51%; specificity = 85% [9]
- Katz hand diagram (click here for image)
- Electrodiagnostics
- **For a more detailed electrodiagnostic review of carpal tunnel syndrome, click here.
- Nerve conduction studies (median sensory and motor) – setup description and photos here
- Median sensory and motor NCS: Sensitivity = 85%; Specificity = 95%
- If the median sensory is abnormal, test the ulnar sensory to make sure this isn’t a polyneuropathy
- If the median sensory is normal, perform the combined sensory index (CSI) – numb thumb, split ring, P8 (details here)
- Needle electromyography (EMG)
- Used to evaluate for axonal degeneration of the motor fibers in the median nerve (will see positive sharp waves and fibrillations)
- Also used in the rest of the ipsilateral upper extremity to rule out other possible diagnoses.
- Not performed unless the patient has signs/symptoms that could be from another pathology.
- Grading the severity of electrodiagnostically-confirmed CTS
- Negative CTS = Normal findings on all tests
- Borderline mild CTS = Abnormal findings only on comparative or CSI tests (side-to-side comparison with ulnar sensory, or CSI tests)
- Mild CTS = Slow median sensory with normal distal motor latency
- Moderate CTS = Slow median sensory AND distal motor latency
- Severe CTS = Absent sensory and increased motor latency
- Profoundly severe CTS = Absent sensory and motor response
- MRI resonance imaging
- Median nerve signal intensity, transverse carpal ligament bowing, and other measurements of the carpal tunnel has a very high sensitivity [10]
- Also useful if a space-occupying lesion is the suspected cause of the CTS
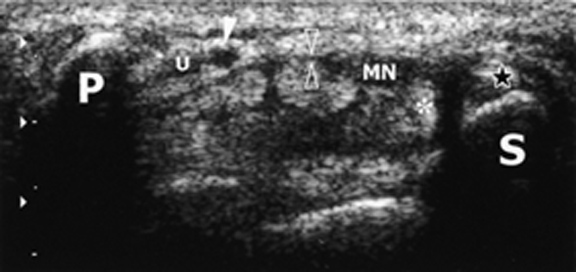
- Ultrasound (image of carpal tunnel here – excellent!)
- A study in 2009 showed that sonographic measurement of the median nerve cross-sectional area (CSA) at the tunnel inlet is a good alternative to NCS as the initial diagnostic test for CTS, but it cannot grade the severity of CTS as well as NCS. [11]
Natural History of CTS
- 1/3 of hands mid and moderate cases improve [27]
- In another study of 132 patients that received no treatment at all, 47.6% recovered, 28.8% remained stable, 23.4% worsened [28] — two-year followup
- Nerve conduction study results mostly either stayed the same or improved
- Remission rates are highest in young females, and pregnant women.
Treatment (Non-Surgical)
- Always start with a conservative approach unless motor deficits and severe sensory or electrodiagnostic abnormalities are present.
- Corticosteroid injections (carpal tunnel injection image and technique)
- More effective than placebo (saline) injections in the short-term, but not at a 12-month follow-up [12]
- Note: they only used 10-mg of kenalog, not the 40mg typically used in clinical practice, so the results may have been even better.
- Another study found that steroid injections and wrist splinting are effective for relief of mild-moderate carpal tunnel syndrome symptoms but have a long-term effect in only 10 percent of patients (those with symptom duration less than 3 months and no thenar atrophy). [15]
- This study gave patients three injections of betamethasone throughout the year, not just a single injection.
- Many other studies have demonstrated clinical efficacy for months, but not an entire year.
- Keep in mind that corticosteroid injections can be repeated when symptoms return.
- Dosing matter!
- A study in 2006 looked at the efficacy of different doses of Depo-Medrol. [16] In the 20, 40 and 60 mg treatment groups, 56%, 53% and 73% of the patients respectively were free of important symptoms at six months follow-up. Also, fewer patients in the 60-mg group went on to get surgery within a 12-months.
- More effective than placebo (saline) injections in the short-term, but not at a 12-month follow-up [12]
- Oral Corticosteroids
- Multiple studies have shown that oral steroids are less effective than injected steroids (into the carpal tunnel)
- Better than placebo — with dose of 20-mg prednisolone daily for 2 weeks, followed by 10-mg daily for 2 weeks [17]
- Corticosteroid Iontophoresis
- Six sessions of 0.4% dexamethasone was not effective in the treatment of mild to moderate CTS [13]
- Wrist splints (image of neutral wrist splint)
- Use a neutral wrist splint, instead of a cock-up (extension) splint [20]
- Advised to tell patients to use only at night, because daytime use interferes with normal activities and the patient is therefore more likely to discontinue use all together
- Nighttime-only use of a neutral wrist splint was shown to be significantly more effective than doing nothing in patients with mild, recent onset CTS [14]
- NSAIDs
- No better than placebo [17]
- Diuretics
- No studies have shown any clinical benefit
- Yoga
- In one trial involving 51 people yoga significantly reduced pain after eight weeks compared with wrist splinting. [18] [19]
- Carpal mobilization
- In one trial involving 21 people carpal bone mobilisation significantly improved symptoms after three weeks compared to no treatment. [18]
- Pyroxidine (B6)
- In two trials involving 50 people, vitamin B6 did NOT significantly improve overall symptoms. [18]
- Ergonomic keyboards
- Two trials involving 105 people compared ergonomic keyboards versus control and demonstrated equivocal results for pain and function. [18]
- Ultrasound
- Short to medium term benefits due to ultrasound treatment in patients with mild to moderate idiopathic carpal tunnel syndrome [21]
- 20 sessions of ultrasound (active) treatment (1 MHz, 1.0 W/cm2, pulsed mode 1:4, 15 minutes per session). Daily for two weeks, then twice a week for 5 weeks.
- Short to medium term benefits due to ultrasound treatment in patients with mild to moderate idiopathic carpal tunnel syndrome [21]
- Trials of magnet therapy, laser acupuncture, exercise or chiropractic care did NOT demonstrate symptom benefit when compared to placebo or control. [18]
Treatment (Surgical)
- Indications
- Patients who fail conservative methods, or have severe sensory deficits, or muscle atrophy.
- The major difference with the medical approach is that surgical transverse carpal ligament release (CTR) has very good long-term results, with very low recurrence rates. [25]
- Efficacy
- A 2007 review of 209 studies showed: [26]
- 75% – complete resolution of symptoms, or only mild residual symptoms
- 17% – mild improvement or no change
- 8% – worsening of symptoms
- Best results are seen in patients with moderate NCS readings [42]
- A 2007 review of 209 studies showed: [26]
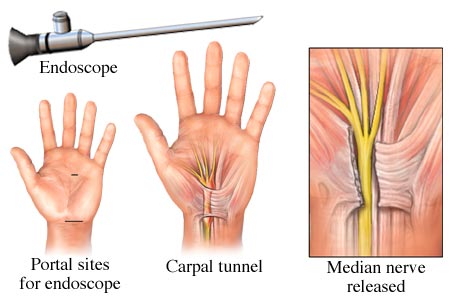
- Open vs Endoscopic release [22] (image of endoscopic carpal tunnel release)
- Patient satisfaction was equal (84-89%)
- Open method had longer return to work (median, 28 days, compared with 14 days )
- Equal benefits (between the two techniques)
- Surgical vs splinting
- A significant proportion of people treated with splinting-only will require surgery [23]
- Diabetics
- Patients with diabetes have the same beneficial outcome after carpal tunnel release as nondiabetic patients. [24]
- Pregnant women should postpone surgery because symptoms frequently resolve completely soon after delivery.
————————————————————————————-
REFERENCES:
1 – Atrosh et al. “Prevalence of carpal tunnel syndrome in a general population.“ JAMA. 1999 Jul 14;282(2):153-8.
2 – Tanaka et al. “The US prevalence of self-reported carpal tunnel syndrome: 1988 National Health Interview Survey data.” Am J Public Health. 1994 Nov;84(11):1846-8.
3 – Margolis W, Kraus JF. “The prevalence of carpal tunnel syndrome symptoms in female supermarket checkers.” J Occup Med. 1987 Dec;29(12):953-6
4 – Tanaka et al. “Prevalence and work-relatedness of self-reported carpal tunnel syndrome among U.S. workers: analysis of the Occupational Health Supplement data of 1988 National Health Interview Survey.” Am J Ind Med. 1995 Apr;27(4):451-70.
5 – Katz JN, Stirrat C, Larson MG, et al. “A self-administered hand symptom diagram in the diagnosis and epidemiologic study of carpal tunnel syndrome.” J Rheumatol. 1990;17:1495-1498.
6 – Amirfeyz et al. “Katz and stirrat hand diagram revisited.” Hand Surg. 2010;15(2):71-3
7 – Novak et al. “Provocative sensory testing in carpal tunnel syndrome.” The Journal of Hand Surgery. Volume 17, Issue 2, April 1992, Pages 204-208
8 – Bruske et al. “The usefulness of the Phalen test and the Hoffmann-Tinel sign in the diagnosis of carpal tunnel syndrome.” Acta Orthopaedica Belgica 2002, N° 2 (Vol. 68/2) p.141
9 – D’Arcy CA, McGee S. “The rational clinical examination. Does this patient have carpal tunnel syndrome?” JAMA. 2000 Jun 21;283(23):3110-7.
10 – Britz et al. “Carpal tunnel syndrome: correlation of magnetic resonance imaging, clinical, electrodiagnostic, and intraoperative findings.” Neurosurgery. 1995 Dec;37(6):1097-103
11 – Moran et al. “Sonographic measurement of cross-sectional area of the median nerve in the diagnosis of carpal tunnel syndrome: correlation with nerve conduction studies.” J Clin Ultrasound. 2009 Mar-Apr;37(3):125-31
12 – Peters-Veluthamaninga et al. “Randomised controlled trial of local corticosteroid injections for carpal tunnel syndrome in general practice.” BMC Fam Pract. 2010 Jul 29;11:54
13 – Amirjani et al. “Corticosteroid iontophoresis to treat carpal tunnel syndrome: a double-blind randomized controlled trial.” Muscle Nerve. 2009 May;39(5):627-33
14 -Premoselli et al. “Neutral wrist splinting in carpal tunnel syndrome: a 3- and 6-months clinical and neurophysiologic follow-up evaluation of night-only splint therapy.” Eura Medicophys. 2006 Jun;42(2):121-6
15 – Graham et al. “A prospective study to assess the outcome of steroid injections and wrist splinting for the treatment of carpal tunnel syndrome.” Plast Reconstr Surg. 2004 Feb;113(2):550-6
16 – Dammers et al. “Injection with methylprednisolone in patients with the carpal tunnel syndrome: a randomised double blind trial testing three different doses.” J Neurol. 2006 May;253(5):574-7
17 – Chang et al. “Oral drug of choice in carpal tunnel syndrome.” Neurology. 1998 Aug;51(2):390-3
18 – O’Connor et al. “Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome.” Cochrane Database Syst Rev. 2003;(1):CD003219
19 – Garfinkel et al. “Yoga-based intervention for carpal tunnel syndrome: a randomized trial.” JAMA. 1998 Nov 11;280(18):1601-3
20 – Burke et al. “Splinting for carpal tunnel syndrome: in search of the optimal angle.” Arch Phys Med Rehabil. 1994 Nov;75(11):1241-4
21 – Ebenbichler et al. “Ultrasound treatment for treating the carpal tunnel syndrome: randomised “sham” controlled trial.” BMJ. 1998 Mar 7;316(7133):731-5
22 – Brown et al. “Carpal tunnel release. A prospective, randomized assessment of open and endoscopic methods.” J Bone Joint Surg Am. 1993 Sep;75(9):1265-75
23 – Verdugo et al. “Surgical versus non-surgical treatment for carpal tunnel syndrome.” Cochrane Database Syst Rev. 2003;(3):CD001552
24 – Thomsen et al. “Clinical outcomes of surgical release among diabetic patients with carpal tunnel syndrome: prospective follow-up with matched controls.” J Hand Surg Am. 2009 Sep;34(7):1177-87
25 – Keiner et al. “Long-term follow-up of dual-portal endoscopic release of the transverse ligament in carpal tunnel syndrome: an analysis of 94 cases.” Neurosurgery. 2009 Jan;64(1):131-7
26 – Bland. “Treatment of carpal tunnel syndrome.” Muscle Nerve. 2007 Aug;36(2):167-71
27 – Padua et al. “Natural history of carpal tunnel syndrome according to the neurophysiological classification.” Ital J Neurol Sci. 1998 Dec;19(6):357-61
28 – Ortiz-Corredor et al. “Natural evolution of carpal tunnel syndrome in untreated patients.” Clin Neurophysiol. 2008 Jun;119(6):1373-8
29 – Padua et al. “Incidence of bilateral symptoms in carpal tunnel syndrome.” J Hand Surg Br. 1998 Oct;23(5):603-6
30 – Lim et al. “The role of wrist anthropometric measurement in idiopathic carpal tunnel syndrome.” J Hand Surg Eur Vol. 2008 Oct;33(5):645-7
31 – Stevens et al. “The frequency of carpal tunnel syndrome in computer users at a medical facility.” Neurology. 2001 Jun 12;56(11):1568-70.
32 – Andersen et al. “Computer use and carpal tunnel syndrome: a 1-year follow-up study.” JAMA. 2003 Jun 11;289(22):2963-9
33 – Rempel et al. “Intensive keyboard use and carpal tunnel syndrome: Comment on the article by Atroshi et al.” Arthritis Rheum. 2008 Jun;58(6):1882-3
34 – Atroshi et al. “Carpal tunnel syndrome and keyboard use at work: a population-based study.” Arthritis Rheum. 2007 Nov;56(11):3620-5
35 – Finsen et al. “Carpal tunnel syndrome during pregnancy.” Scand J of Plas and Reconst Surg and Hand Surg 2006, Vol. 40, No. 1 , Pages 41-45
36 – Padua et al. “Systematic review of pregnancy-related carpal tunnel syndrome.” Muscle Nerve. 2010 Nov;42(5):697-702
37 – Niempoog et al. “Local injection of dexamethasone for the treatment of carpal tunnel syndrome in pregnancy.” J Med Assoc Thai. 2007 Dec;90(12):2669-76
38 – Sharifi-Mollayousefi et al. “Assessment of body mass index and hand anthropometric measurements as independent risk factors for carpal tunnel syndrome.” Folia Morphol (Warsz). 2008 Feb;67(1):36-42
39 – Caliandro et al. “Distribution of paresthesias in Carpal Tunnel Syndrome reflects the degree of nerve damage at wrist.” Clin Neurophysiol. 2006 Jan;117(1):228-31
40 – Chan et al. “The relationship between electrodiagnostic findings and patient symptoms and function in carpal tunnel syndrome.” Arch Phys Med Rehabil. 2007 Jan;88(1):19-24
41 – Sawaya et al. “When is the Phalen’s test of diagnostic value: an electrophysiologic analysis?” J Clin Neurophysiol. 2009 Apr;26(2):132-3
42 – Bland JD. “Do nerve conduction studies predict the outcome of carpal tunnel decompression?” Muscle Nerve. 2001 Jul;24(7):935-40









")


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
I have found the solution to my carpal tunnel ailments… and they work. I’ve been using various braces, medications, therapies and exercises and I promise you – nothing works better than the aPallo Day and Night Wrist Braces. I can work without pain and I’m ecstatic to share!
http://www.palomedical.com/educational-videos/apallo-wrist-brace-system/apallo-wrist-brace-system-day-brace/
http://www.palomedical.com/educational-videos/apallo-wrist-brace-system/apallo-wrist-brace-system-night-brace/
Normally I don’t allow direct links to products, but these look like great carpal tunnel braces. I’d love to have a couple to try out.