Posted by Azlan Tariq, D.O.
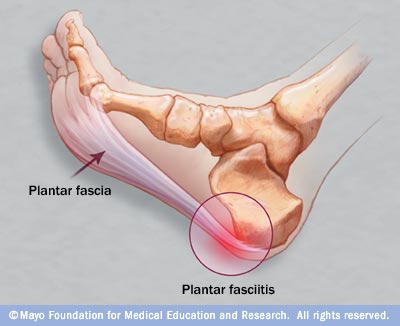
Plantar fasciitis is a painful inflammatory process of the plantar fascia.
Epidemiology:
- Most common cause of inferior heel pain and 11-15% of all foot pain
- Common among runners and military personnel.
- Incidence peak between 40-60 years.
- Link to gender unclear but some studies show women affected twice as often as men
- BILATERAL IN 1/3rd of cases. Bilateral presentation appears in association with some seronegative spondyloarthropathies.
Pathological features:
- Abnormality near the site of origin of the plantar fascia at medial tuberosity of calcaneus.
- Degenerative and chronic inflammatory changes seen with or without fibroblastic proliferation.
Risk Factors:
- Poorly understood. Multifactoral.
- Risk factors include obesity, occupations that require prolonged standing, pes planus (flat feet), reduced ankle dorsiflexion and inferior calcaneal exostoses (heel spurs).
Limited or absent data on the following risk factors
- Running excessively
- Suddenly increasing length of runs
- Wearing faulty running shoes
- Running on unyielding surfaces
- Having high aches (pes cavus)
Clinical course:
- 80% of patients have resolution of symptoms within 12 months
Clinical Diagnosis:
- Clinical assessment alone usually sufficient.
- Symptoms
o Gradual onset pain in inferior heel
o Worse with 1st step in morning or period of inactivity
o Pain improves with gradually increasing activity but worse end of the day
o Often localized area of maximal tenderness over anteromedial aspect of inferior heel
o Limitation of ankle dorsiflexion due to tight Achilles tendon
- ICD-9 code: 728.71 “plantar fascial fibromatosis”
- ICD-10 code: M72.2 “plantar fascial fibromatosis”
Imaging:
- Should be used if need to rule out calcaneal stress fracture or other rare bony lesions
- Heel spurs are of no value in either confirming or ruling out diagnosis
- Bone scan positive in 60-98 percent of cases with plantar fasciitis.
- Ultrasound is useful. Marked increase in thickness of plantar fascia seen etc
Treatment:
- Early initiation of conservative treatment (within 6 weeks) after onset believed to hastens recovery
o Physical therapy
- No strong evidence that stretching calf, taping, strapping foot, ice, heat or massage works.
- No benefit of magnetic insoles
- No significant benefit of ultasonography, laser treatment or iontophoresis.
o Orthotic devices
- No data on efficacy of devices as compared to placebo or no treatment. Available data is limited or conflicting.
- Low-cost prefabricated ethylene vinyl acetate (EVA may be more beneficial than custom-made ones in uncomplicated plantar fasciitis per randomized controlled study. 1
o Splinting and walking casts
- Conflicting results of trials where night splints were used.
- No published data from controlled trials of immobilization with casts.
o Anti-inflammatory agents
- Limited data suggests that injection of corticosteroids provides short term pain relief.
- Trial with 91 patients showed that injecting steroids + anesthetic resulted in significantly greater improvement in pain at one month than local anesthetic alone.
Learn about the plantar fascia steroid injection technique and tips HERE.
o Botox
- Botulinum toxin type A injection seems to produce significant improvements in pain relief and overall foot function according to a short-term, randomized, controlled, double-blinded study. 2
o Extracorporeal shock-wave therapy
- Thought to stimulate healing of soft tissue and inhibit pain receptors
- Of the 6 studies, 3 showed no benefit, 2 showed minimal benefit, while 6th study showed significant reduction in pain on first walking in the morning at 6 months.
o Orthopedic Surgery
- May be considered for small subgroup of patients with persistent, severe symptoms without resolution for at least 6 to 12 months
- Favorable outcomes in 75% of patients. Recovery time could be months. Closed procedures have more rapid recovery and resumption of usual activities although risk of nerve injury higher.
Prevention:
- Trial with 390 army recruits showed that improved shock absorption resulted in significantly lower incidence of injuries.
Ultrasound:
- One study showed that ultrasound-guided corticosteroid injection resulted in complete resolution in 4 out of 5 heels with a 24 week mean duration of follow up.3
- One study showed that ultrasound-guided corticosteroid injections had the same outcome as injections administered with palpation guidance.4
- One study showed that patients injected with 7-mg of betamethasone and 0.5-ml of 1% lidocaine with ultrasound guidance had a significant improvement in VAS score. Plantar fascia thickness was noticed to be decreased significantly 3 months after injection. 5
CONCLUSION
- Plantar fasciitis is self-limiting. More than 80% of cases will resolve within one year regardless of therapy
- Even though there is limited evidence, start with low-risk, cheap interventions such as stretching calf muscles, stretching plantar fascia on waking up, avoid flat shoes, using OTC arch support/heel cushions, limiting extended physical activities. TRIAL OF NSAIDs MAY BE REASONABLE.
- Corticosteroid injections CAN provide short term benefit.
- Uncertain evidence of use of custom-made orthotic devices, night splints and casting.
- Surgery should be reserved for patients in whom conservative therapy has not helped after 6-12 months.
1) Baldassin V, Gomes CR, Beraldo PS. Effectiveness of prefabricated and customized foot orthoses made from low-cost foam for noncomplicated plantar fasciitis: a randomized controlled trial. Arch Phys Med Rehabil. April 2009;90(4):701-706.
2) Babcock MS, Foster L, Pasquina P, et al. Treatment of pain attributed to plantar fasciitis with botulinum toxin A: a short-term, randomized, placebo-controlled, double-blind study. Am J Phys Med Rehabil. Sep 2005;84(9):649-54
3) Kane D, Greaney T, Bresnihan B, Gibney R, FitzGerald O. et al. Ultrasound guided injection of recalcitrant plantar fasciitis. Ann Rheum Dis. 1998 Jun;57(6):383-4.
4) Kane D, Greaney T, Shanahan M, et al. The role of ultrasonography in the diagnosis and management of idiopathic plantar fasciitis. Rheumatology (Oxford) 2001;40: 1002-8.
5) Tsai WC, Wang CL, Tang FT, Hsu TC, Hsu KH, Wong MK. Treatment of proximal plantar fasciitis with ultrasound-guided steroid injection. Arch Phys Med Rehabil. 2000 Oct;81(10):1416-21.










")


{kind=link}
Do you perform the plantar fascia injection from the plantar heel straight up, or from the side?
We perform the injection through the posterior heel parallel to
the long axis of the ultrasound transducer.
https://thepainsource.com/wp-content/uploads/2010/09/Capture.jpg